When someone arrives at an emergency room with stroke symptoms, the clock is already running. Brain tissue dies at a rate of roughly 1.9 million neurons per minute during an ischemic stroke. The only way to stop that damage is to quickly confirm the type of stroke and begin the appropriate treatment. Today, Advanced Stroke Imaging plays a critical role in that process, helping ER teams rapidly identify the cause of symptoms, distinguish between stroke types, and make life-saving treatment decisions when every second counts.
Stroke imaging ER protocols have become the single most important factor in determining how quickly patients receive treatment. The speed and accuracy of the initial scan shapes every decision that follows: which medication to give, whether a clot retrieval procedure is needed, and whether the patient still has salvageable brain tissue worth fighting for.
Why Advanced Stroke Imaging Determines Outcomes
A stroke occurs when blood flow to the brain is interrupted. In an ischemic stroke (roughly 87% of all strokes), a blood clot blocks an artery supplying the brain. In a hemorrhagic stroke, a blood vessel ruptures and bleeds into surrounding tissue. The treatments for these two types are opposite: clot-dissolving drugs save lives in ischemic strokes but can be fatal in hemorrhagic ones.
That is why stroke diagnosis technology centers on imaging. No physical exam, blood test, or symptom checklist can reliably distinguish between a clot and a bleed. Only a brain scan can.
Three time-sensitive realities drive the urgency:
- Clot-dissolving medication (tPA) must be given within 4.5 hours of symptom onset for most patients
- Mechanical clot retrieval (thrombectomy) works best within 6 hours, though advanced imaging has extended this window to 24 hours in select cases
- Every 15-minute reduction in treatment delay improves the odds of a good functional outcome
Modern emergency stroke treatment protocols aim for a “door-to-needle” time of under 60 minutes, with top-performing centers targeting under 30.
How ERs Use CT Scans to Diagnose Strokes
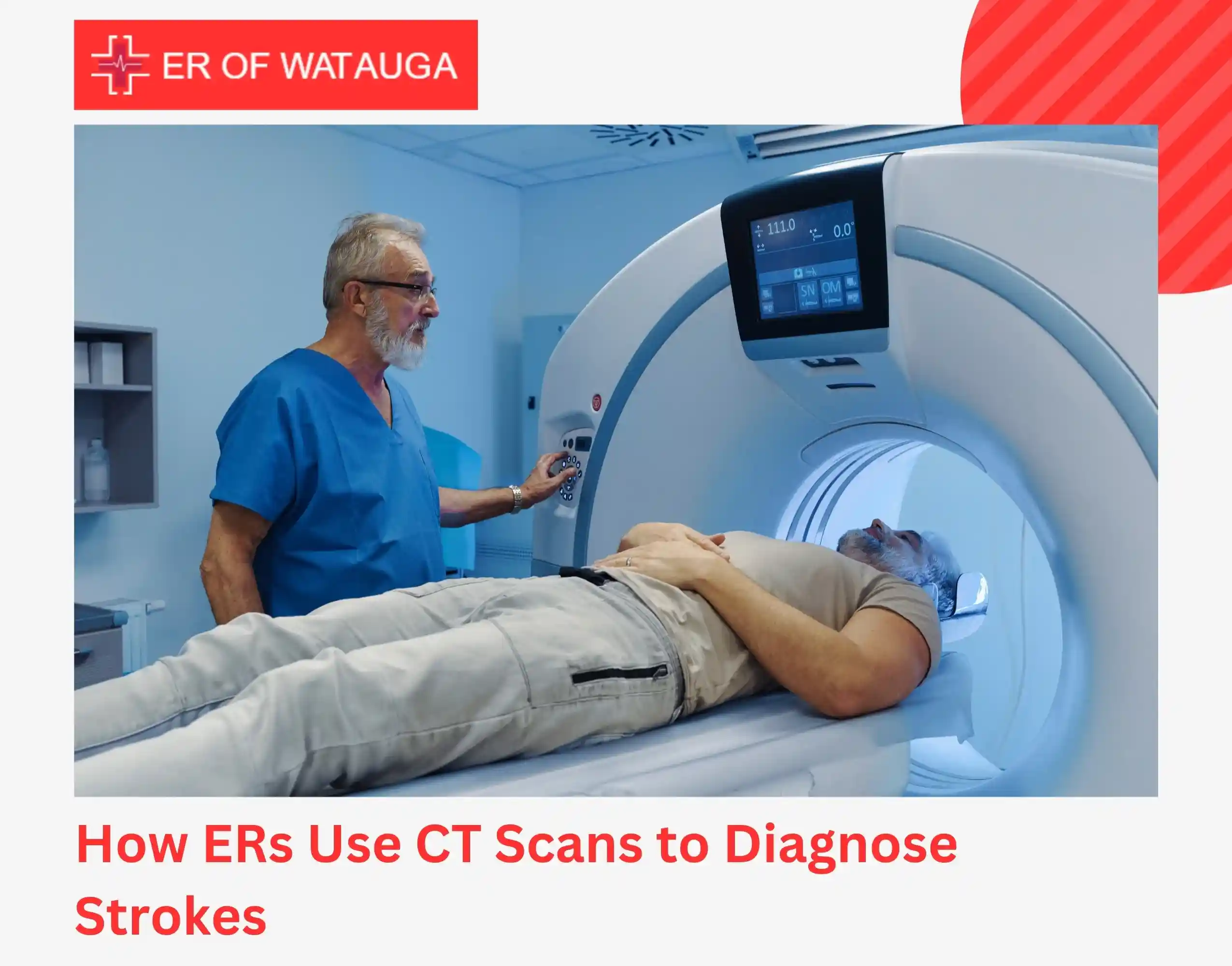
The CT scan stroke protocol is the backbone of every ER stroke evaluation. A non-contrast CT scan is typically the first test performed, often within minutes of arrival. It is fast, widely available, and answers the most urgent question: is the patient bleeding?
Non-Contrast CT
A standard CT scan of the head takes less than a minute. It can identify hemorrhagic stroke immediately by showing areas of active bleeding. For ischemic stroke, early signs may be subtle on a plain CT, but the scan’s primary value is ruling out hemorrhage so that clot-dissolving treatment can proceed safely.
This speed is why the CT scan stroke protocol remains the global standard for initial stroke workup. No other imaging modality matches it for rapid hemorrhage detection.
CT Angiography (CTA)
CT angiography is typically performed immediately after the non-contrast CT, often during the same scanner session. A contrast dye is injected intravenously, and the scan maps the blood vessels from the aortic arch through the brain.
CTA answers the next critical question: where is the blockage? It identifies large vessel occlusions, the type of clot most likely to benefit from thrombectomy. Without CTA, physicians would be guessing whether a patient needs a clot retrieval procedure or medication alone.
CTA has become a standard part of stroke imaging ER workflows in most emergency departments because it adds only minutes to the evaluation while dramatically improving treatment decisions.
CT Perfusion Imaging
CT perfusion takes the evaluation one step further by measuring actual blood flow through brain tissue. It distinguishes between two zones:
- Core infarct: Brain tissue that has already died and cannot be saved
- Penumbra: Tissue that is oxygen-starved but still alive, the territory that treatment aims to rescue
This distinction matters most for patients who arrive outside the traditional treatment window. If a large penumbra remains, emergency stroke treatment may still be worthwhile even 6 to 24 hours after symptom onset. If the core infarct has already consumed most of the affected territory, aggressive intervention carries more risk than benefit.
CT perfusion has fundamentally changed stroke diagnosis technology by shifting decisions from clock-based rules to tissue-based evidence.
What Happens During a Stroke Evaluation: Step by Step

The ER stroke evaluation follows a tightly sequenced protocol where every minute is tracked.
1. Immediate assessment
The patient is assessed for stroke warning signs using a standardized neurological scale. Vital signs including blood pressure are measured. An IV line is placed and blood is drawn for labs.
2. Non-contrast CT scan
The CT scan stroke protocol is activated immediately. Results are interpreted in real time, often by the emergency physician at the scanner.
3. CT angiography
If the non-contrast CT shows no hemorrhage, CTA is performed to locate any vessel occlusion. This step determines whether the patient is a candidate for thrombectomy.
4. Treatment decision
Based on imaging, the team decides between IV thrombolysis (clot-dissolving medication), thrombectomy referral, or supportive management. In some cases, CT perfusion is added to guide decisions for late-presenting patients.
5. Treatment initiation
If thrombolysis is indicated, the medication is started immediately. If thrombectomy is needed, the ER team stabilizes the patient and coordinates rapid transfer to a comprehensive stroke center with interventional neurology capabilities.
The goal of stroke imaging ER protocols is to compress this entire sequence into the shortest possible timeframe. In practice, the imaging itself takes minutes. The delays that cost patients brain tissue usually happen before arrival or during transitions between care steps.
The Role of Freestanding ERs in Stroke Care
Freestanding emergency rooms like ER of Watauga play a specific and important role in the stroke treatment chain. We are often the closest emergency facility, which means we are the first point of contact when stroke symptoms appear.
Our role in emergency stroke treatment includes:
- Rapid CT scanning to confirm or rule out hemorrhage within minutes of arrival
- Neurological assessment using standardized stroke scales
- Blood pressure management and medical stabilization
- Administration of IV thrombolysis when appropriate and within the treatment window
- Immediate coordination of transfer to comprehensive stroke centers for patients who need thrombectomy or neurosurgical intervention
- Continuous monitoring during the stabilization and transfer process
Our on-site CT scanner and laboratory allow us to complete the critical first steps of stroke diagnosis technology without the wait times that often delay care in crowded hospital emergency departments. For stroke patients, those saved minutes translate directly into preserved brain function.
We do not perform thrombectomy or neurosurgery. But by diagnosing fast and transferring efficiently, we give patients the best chance of reaching definitive care within the treatment window.
Recognizing Stroke Symptoms: When to Go to the ER
No imaging protocol matters if the patient doesn’t get to the ER in time. Recognizing stroke symptoms and calling 911 immediately is the single most important step in the entire treatment chain.
Use the BE-FAST method:
- Balance: sudden loss of balance or coordination
- Eyes: sudden vision changes in one or both eyes
- Face: one side of the face droops when smiling
- Arms: one arm drifts downward when both are raised
- Speech: slurred or garbled speech, difficulty repeating simple phrases
- Time: note the time symptoms started and call 911 immediately
Other warning signs include sudden severe headache with no known cause, sudden confusion, and sudden numbness or weakness on one side of the body.
Do not drive yourself or wait to see if symptoms improve. Every minute of delay reduces the likelihood of full recovery. Stroke imaging ER evaluation should begin as soon as possible after symptom onset.
If someone near you shows these signs, even briefly, they need emergency evaluation. Transient symptoms that resolve on their own may indicate a TIA (transient ischemic attack), which is a warning that a full stroke may follow.
Key Takeaway
Stroke imaging ER protocols are the reason modern stroke outcomes have improved dramatically over the past decade. A non-contrast CT scan rules out bleeding in under a minute. CT angiography locates the blockage. CT perfusion identifies salvageable brain tissue. Together, these tools give emergency physicians the information they need to act fast and act correctly.
But imaging only works if patients arrive in time. If you or someone near you develops sudden face drooping, arm weakness, speech difficulty, or severe headache, call 911 or get to the nearest ER immediately.
ER of Watauga provides 24/7 emergency stroke evaluation with on-site CT imaging, EKG monitoring, and cardiac enzyme testing to identify stroke risk factors and concurrent cardiac events. Walk in anytime or call 817-427-3939.
[Get Directions to ER of Watauga]
Frequently Asked Questions (FAQs)
1. What is the fastest imaging test for stroke in the ER?
A non-contrast CT scan is the fastest and most widely used initial test for suspected stroke.
2. Why is CT scan preferred over MRI in emergencies?
CT scans are quicker, more accessible, and highly effective at detecting bleeding, making them ideal for urgent decisions.
3. Can stroke be diagnosed without imaging?
No. Imaging is essential to confirm the type of stroke and guide appropriate treatment.
4. How does imaging affect stroke treatment decisions?
Imaging helps determine whether a patient is eligible for thrombolysis or thrombectomy, improving outcomes.
5. How quickly should imaging be done after arriving at the ER?
Guidelines recommend brain imaging within 20 minutes of arrival for suspected stroke patients.